Catheter ablation for atrial fibrillation is now the most frequently performed ablation in the UK and the Western world.
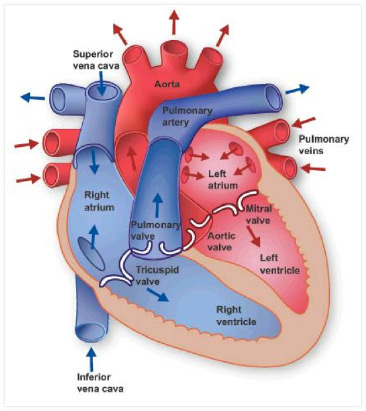
First developed in Bordeaux, France in 1999, doctors there discovered that most episodes of paroxysmal AF ablation are triggered by an extra heartbeat, or ‘ectopic’, from just inside one of the pulmonary veins. The pulmonary veins carry oxygenated blood from the lungs back to the heart, to the chamber called the left atrium (see figure). Cells just inside the entrances to these veins (where they connect to the heart) fire to cause an ectopic, which in turn triggers AF. At first these cells were targeted directly with ablation inside a vein that was firing, but this didn’t work as another vein would just do the same thing later. So a technique called pulmonary vein isolation was developed to get around this. The pulmonary veins usually exist in two pairs of two veins, one pair from each lung. Occasionally three or five veins are present rather than four.
To book a consultation with Dr Segal, about AF ablation in London, get in touch here.
More Information
Pulmonary Vein Isolation
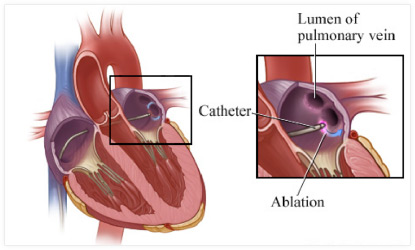
Pulmonary Vein Isolation, or PVI for short, is the process of creating an electrical barrier around the entrance to the pulmonary veins. If this barrier exists, ectopics from cells inside the veins cannot conduct to the left atrium to cause an episode of AF. An analogy is trying to corral horses inside fencing. As long as there are no gaps between the fences, the horses cannot escape. PVI can be performed by creating a barrier around the entrance to each individual vein, called segmental ostial ablation, or it can be performed further out around two veins (one pair of veins) at a time on one side of the atrium. This technique is called wide area circumferential ablation, or WACA. When using radiofrequency catheters, the catheter tip is moved sequentially around the vein entrance building up ablation points until they create a barrier. This is known as point-by-point ablation.
It has been shown in clinical trials that WACA is superior to segmental ablation when using radiofrequency ablation catheters. However, newer technologies have been developed designed to speed up ostial PV isolation, which try to ablate the whole vein entrance in one or two ablation deliveries. These include the cryo-balloon, the Ablation Frontiers PVAC catheter (pulmonary vein ablation catheter), the laser balloon and the nMARQ catheter. All of these catheters are designed to sit at or around the vein entrance and perform segmental isolation. Results from clinical trials have shown that these different technologies currently have approximately equivalent success rates for the treatment of paroxysmal AF.

What if my AF is persistent not paroxysmal?
If you have persistent AF, it means your AF is continuous and means your heart prefers to stay in AF rather than return to normal rhythm. This usually occurs if you are older, have had paroxysmal AF for a long time, you have a big left atrium or if you have other types of heart disease in addition to AF. Often, you will have had paroxysmal AF but one day the AF didn’t go away and it became persistent.
Once the AF is persistent, it means it is not reliant on triggers from the pulmonary veins alone to exist. It means the cellular architecture of the atria (the top chambers of the heart) have become sufficiently distorted that they now prefer to fibrillate. A consequence of this is that performing PVI alone may not be sufficient to cure persistent AF and a more extensive ablation process may be required – although the exact type of ablation necessary is still being debated/evaluated.
Persistent AF Ablation
When performing persistent AF ablation, PVI is still performed first. After this, there is no consensus on the next appropriate step but these include targeting abnormal electrical signals identified in the atria (particularly the left atrium) with ablation. These signals are known as fractionated electrograms and ablation of these signals is called fractionation ablation, or sometimes Complex Fractionated Atrial Electrogram Ablation (or CAFÉ ablation for short). Or lines of ablation can be created to act as barriers to electricity flowing around the atrium to prevent AF. The three commonest lines are the left atrial roofline, the mitral isthmus line and the cavo-tricuspid isthmus line (or right atrial flutter line). Although creating lines and CAFE ablation can cure persistent AF, they can also create circuits for arrhythmia and this is probably why trials of AF ablation have not found them to be helpful overall, but in individual patients, they can still be curative.
Why do so many people need more than one ablation procedure?
Unlike most other types of ablation, AF ablation requires the formation of long lines inside the heart, rather than single points. If even one of the points in a line recovers function (because the body tries to repair the damage after ablation), the barrier becomes incomplete and AF can recur. Using the ‘horses’ analogy, one of the fences will fall over and allow the horses to escape. It is for this reason that 50% of people who have paroxysmal AF ablation and 70% of people with persistent AF ablation require a second procedure and some patients will require 3 or more procedures.
Similarly, the challenge faced in trying to restore normality to the left atrium in someone who has had persistent AF for many months or years it considerable, and multiple ablation procedures can be required.
The ablation procedure
I prefer to perform AF ablation using a general anaesthetic as the procedures are long and can be painful if you are awake, even with sedation. Prior to the ablation itself, a probe is passed into the oesophagus (the gullet or food pipe) to take detailed pictures of the heart using ultrasound (called trans-oesophageal echo, or TOE for short). This ensures there are no clots inside the heart, which would preclude performing ablation.
If the TOE shows the heart is clear of clots, fine plastic tubes are then inserted into the veins at the top of the right leg. Catheters and other instruments can then be passed through these tubes directly up to the heart via the veins inside the body. An x-ray camera guides this process.
To get access to the left atrium, a procedure called a trans-septal puncture is required. This technique aims to create a small hole in the wall, which lies between the two atria, called the inter-atrial septum. Passing a long metal needle up through a long plastic sheath to the septum creates the hole, guided by x-rays and the images from the TOE probe.
Once inside the left atrium, a drug called heparin is given to ‘thin’ the blood to reduce the risk of causing a clot, leading to a stroke. The ablation catheter and a special catheter, called a Lasso catheter, are then advanced into the heart through the hole and can be moved around the left atrium to record electrical information. The Lasso catheter has 20 different electrodes on it, so it can rapidly pick up information and this can be used to create a computerized 3-dimensional ‘map’ or ‘geometry’ of the inside of the left atrium (see figure). Once the geometry has been created, the catheters can be visualised moving around inside it, limiting the need to use x-rays.

Ablation is then performed depending on the chosen technique and the catheters are removed. The sheaths are then removed from the top of the leg and another drug is given to reverse the heparin. This allows clotting to return to normal so that the holes at the top of the leg do not continue to bleed. The TOE probe is removed and the anaesthetic is reversed. Once awake, patients are transferred back to the ward for further monitoring and have to lie flat for up to four hours.
Monitoring continues overnight. Patients are checked the following day and if the puncture sites at the top of the leg have healed and they are mobile, they will be discharged.
Will I know if the ablation is successful straight away
Unfortunately not. Although it is always possible to say if the ablation went well and everything was achieved (e.g. PVI was completed successfully), it does not necessarily mean the AF is cured. This needs to be assessed over a longer period of time, the earliest usually being 2-3 months after the procedure. This is because the lesions that ablation creates, take 2-3 months to mature properly. Some will go on to form a permanent barrier, or scar, while others will heal and allow electricity to conduct again. The latter may result in failure of the procedure and the need for repeat ablation.
Success rates
AF ablation success rates depend on a number of factors. Firstly and mostly importantly is whether the AF is paroxysmal (comes and goes on its own) or is persistent. Generally currently accepted procedural success rates are:
Paroxysmal AF
Chance of cure after 1st procedure – 50%
Chance of cure after 2 or more procedures – 80-90%
Persistent AF
Chance of cure after 1st procedure – 30-40%
Chance of cure after 2 or more procedures – 60-70%
Long-term success rates after AF Ablation (3-5 years) – 50%
If AF recurs years after what appears to have been a successful ablation, repeat ablation is usually indicated. The very long-term outcomes after AF ablation are unknown at this time. It may be that most patients will require repeat ablations every 5 years or so to maintain normal rhythm, or it may prove that ablation will eventually be unsuccessful after a certain period of time. We assume that ablation will, however, be curative after one or two procedures in a proportion of patients.
In addition to type of AF, other critical factors are size of the left atrium and how long AF has been present, if persistent. In general, a left atrium larger than 5cm has a lower chance of success and atria larger than 5.5cm have a very low chance of cure. People with left atria this size are usually not offered ablation. Similarly, if you have been in AF continuously for more than a year, the success rate is lower and people with AF for more than 3 or 4 years have significantly lower success rates. However, I have achieved a successful ablation for a patient who was in AF for more than 30 years!
Conversion of AF into an atrial flutter

Patients with persistent AF can develop a different rhythm to AF after ablation, called atrial flutter. This rhythm is similar to AF in that it is confined to the atria, but is regular rather than irregular and is due to a single rapid re-entry circuit. There are several different types of atrial flutter and the commonest to occur after ablation of persistent AF are those in the left atrium. This is because the lines of scar caused by the ablation leave channels of heart tissue for electricity to conduct through.
From the perspective of the patient who develops flutter after AF ablation, it appears as a setback or complication. It usually requires medical attention and sometimes a hospital visit. However, from an electrophysiologist’s perspective, the development of atrial flutter is seen as a good sign as it means the atria can no longer fibrillate. This implies that the ablation has been successful and if the atrial flutter is then ablated (usually reasonably straightforward), a long-term cure can usually be achieved. An almost identical ablation procedure is required to ablate left atrial flutters. Success rates of ablation of atrial flutter are in the region of 85% for a cure after a single procedure.
Two major types of atrial flutter seen after AF ablation are roof-dependent left atrial flutter and mitral isthmus reentry. The figures below show the re-entrant circuits of these two rhythms within the left atrium. Creating a line of ablation at the left atrial roof, or at the mitral isthmus will cure these rhythms, respectively.
Complications
As with any heart procedure or operation, complications can occur. The current generally accepted overall complication rate for any type of AF ablation is 3-4% – in other words, up to 4 in 100 people undergoing AF ablation will experience a complication.
Outlined below is a comprehensive list of all complications, which can occur with AF ablation:
1. Vascular injury
Risk of it happening: 1 in 25 to 50 (2-4%)
The veins at the top of the leg are used as conduits to feed ablation catheters to the heart. So there are several locations where injury may occur. The commonest by far is at the puncture site in the groin, called the femoral vein. Although veins themselves are rarely injured, they lie adjacent to arteries that are more likely to be. Injury to an artery causes a weakness in the artery wall, which can bulge outwards to form what is called a pseudo-aneurysm. This can show itself by a painful swelling at the top of the leg after ablation and is diagnosed by ultrasound scan. Treatment requires bed rest and often injection of the aneurysm with a drug called thrombin. The drug causes the blood inside it to clot and takes pressure off the artery wall, allowing it to recover. Surgery to the artery is required if this is unsuccessful or not appropriate.
Other veins can also be damaged deeper inside the body. Injury to these larger veins can cause bleeding into what is called the retro-peritoneal space. This is the space behind the abdomen but in front of the spine. This typically causes back pain and low blood pressure and is usually diagnosed by a CT scan of the abdomen. If confirmed, it may require treatment in the form of angioplasty to a vein (blowing up a balloon at the site of the leak) and deploying a covered stent (a metal cage covered in material to prevent further leaking). Rarely surgery can be required.
2. Cardiac perforation + tamponade
Risk of it happening: 1 in 50 (2%)
This is when the ablation catheter inadvertently makes a small hole in the wall of the heart causing blood to leak out into the sack around the heart called the pericardium. If only a small amount of fluid accumulates, it can be left. If not, it requires insertion of a drain into the pericardium using a needle inserted under the ribs. The drain is usually only necessary for 24 hours.
3. Cardiac surgery
Risk of it happening: 1 in 300 (0.3%)
Cardiac surgery is required if cardiac perforation and tamponade occurs and does not settle after inserting a drain.
4. Stroke
Risk of it happening: <1%
This can be a temporary or permanent stroke and can be mild or very large. It usually occurs within 24 hours of the procedure. Stroke occurs rarely now ablation is performed with patients fully anticoagulated.
5. Atrio-oesophageal fistula
Risk of it happening: 1 in 1000 (0.1%)
This very rare complication is when a hole is created between the back wall of the atrium, which connects to the oesophagus (or food pipe) behind it. This can cause blood to leak out of the heart into the pericardium or oesophagus and can also allow air and stomach contents to leak into the heart (which can then travel to the brain to cause a stroke). It may not be evident immediately after the ablation but can cause chest pain. The treatment, if suitable, is usually surgery, but death is unfortunately common after this rare complication.
6. Dying
Risk of it happening: 1 in 1000 (0.01%)
Death is rare after AF ablation and can occur with large strokes, atrio-oesophageal fistula or bleeding that cannot be controlled with surgery.
7. Pulmonary vein stenosis
Risk of it happening: <<1%
This is when the entrance to a pulmonary vein becomes narrowed, or even completely blocked, after ablation. This process usually takes weeks or months to develop. Fortunately, it is very rare with current technologies and methods. By performing ablation away from the entrance to the veins (using the WACA approach – see above), it is highly unlikely to occur. It causes breathlessness or haemoptysis (coughing up blood). It is treated by inserting a stent, or it can require surgery.
8. Phrenic nerve palsy
Risk of it happening: <1%-4%
The nerve that supplies the diaphragm runs behind the back of the heart. In some cases this can be injured when performing ablation. The diaphragm stops moving if the nerve stops working and this causes breathlessness. The nerve does eventually recover in the vast majority of people but this can take weeks, and rarely months, or even up to a year. It is very rare after point-by-point ablation. However, it is well known with the use of the cryo-balloon, the ablation frontiers PVAC catheter, the laser balloon and the nMARQ catheter. The risk for these latter technologies is reported between 1 and 4%.
9. Heart block and pacemaker
Risk of it happening: <1%
This complication should only occur with ablation of persistent AF, and not PVI alone. It can occur during ablation of CAFÉs (see above) within the left or right atrium, which are close to the mitral or tricuspid valve in the middle of the heart. This is also where the hearts normal conduction system lies and so can be damaged inadvertently. If damaged it can result in heart block, which means electrical signals cannot travel from the atria to the ventricles. This causes bradycardia or a slow heart beat. A permanent pacemaker needs to be fitted if this does not recover, usually assessed 24-48 hours later. This complication does not mean the procedure cannot still be successful and sometimes the creation of heart block is actually beneficial (although not usually first choice).
10. Oesophageal perforation
Risk of it happening: <1 in 1000
This is when a hole is created in the oesophagus, or food pipe/gullet, and occurs rarely on trying to insert the TOE probe at the beginning of the procedure. It is more likely to occur if you have an oesophageal stricture, or narrowing of the oesophagus. So if you have problems swallowing food, it is important to mention this. This complication causes chest pain and often requires surgery to the oesophagus, which is a major operation. If it occurs, you will be unable to eat and drink until it has recovered completely. Although this complication is very rare, it is not uncommon for people to die from complications related to it.
11. Pneumothorax
Risk of it happening: <1%
A pneumothorax is collapse of the lung due to injury to it’s lining. Occasionally it proves impossible to introduce the catheters from the veins at the top of the leg and one of them has to be placed from a vein just under the left collarbone or from a vein in the neck. The needle used to access these veins can inadvertently injure the lining of the lung causing the pneumothorax. It causes breathlessness or chest pain and is usually easily diagnosed on chest x-ray. The treatment depends on how much the lung collapses. Small collapses can simply be monitored and will heal on their own. Larger collapses require insertion of a fine drain between the ribs to allow the lung to expand. This can usually be removed after a day or two. Rarely surgery is necessary to repair the hole in the lung lining.
Follow up after ablation
It is quite common to get episodes of AF in the first few weeks after ablation – this is an effect of the heart adapting to the effects of the new ablation lesions. This should settle by 6-8 weeks and recurrences of AF after this imply the procedure has not been successful. Sometimes AF won’t recur until anti-arrhythmic drugs are stopped. In either case, repeat ablation is the preferred option. If AF does not recur after stopping medication, monitoring is continued with periodic heart monitors and ECGs. AF can return at any time after ablation, even years later and so further ablation may be indicated at that time.
All patients need to have their blood thinned for a period after ablation. If you needed warfarin (or similar drug) before the procedure i.e. your CHADS-VASc score is 1 or more (see section on AF for meaning of CHADS-VASc score), it is continued even after a successful ablation. This is to ensure people are protected from a stroke if AF returns unexpectedly, even years later. In low risk patients (CHADS-VASc score 0) it is reasonable to stop these drugs two weeks after the procedure.